
Many patients ask this important question before a thyroid cancer biopsy: “Can a biopsy cause cancer to spread?” As a thyroid cancer specialist, the honest, evidence-based answer is that biopsy-related cancer spread is extremely rare. For most patients, the risk of delaying diagnosis is much greater than the small theoretical risk of tumor seeding.
A biopsy helps doctors confirm whether a lump, thyroid nodule, mouth ulcer, neck swelling, or suspicious growth is cancerous. Without diagnosis, treatment planning becomes uncertain. The American Cancer Society notes that biopsy is often the best way to know whether cancer is present, and the chance of spread during biopsy is extremely rare.
This article explains the truth, myths, benefits, and safety of biopsy, especially for patients looking for a thyroid doctor, thyroid evaluation, or thyroid cancer treatment in Nepal.
Quick Answer: Can a Biopsy Spread Cancer?
In most cases, no. A biopsy does not cause cancer to spread.
Very rarely, cancer cells may grow along the path of a biopsy needle. This is called needle tract seeding or tumor seeding. However, major cancer organizations describe this as uncommon, and doctors use standard techniques to reduce risk. The National Cancer Institute states that the chance of surgery or biopsy causing cancer to spread is extremely low when standard procedures are followed.
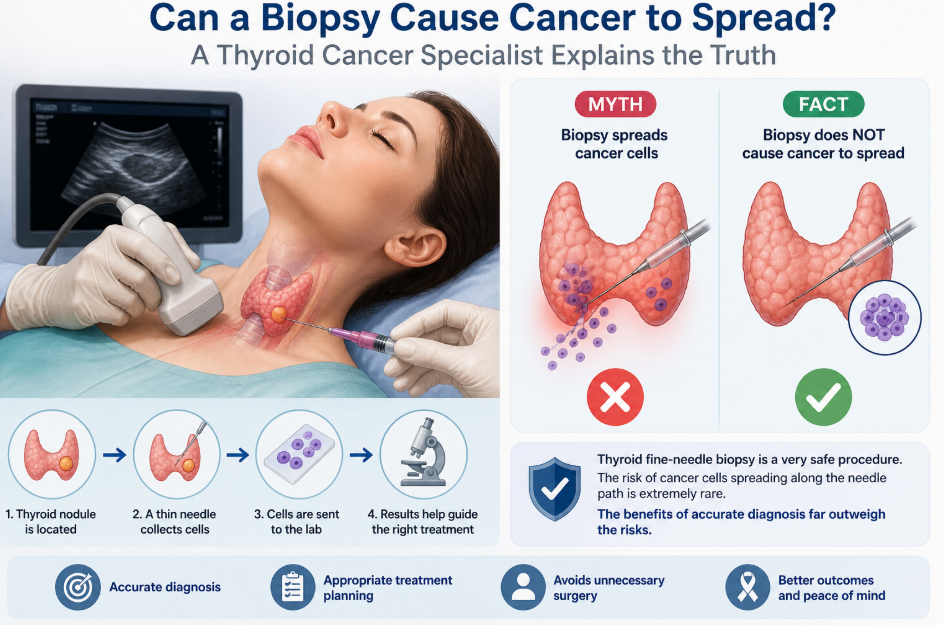
For thyroid nodules, fine needle aspiration biopsy is widely used because it is minimally invasive and helps identify whether a nodule is benign, suspicious, or malignant. Johns Hopkins Medicine describes thyroid fine needle aspiration as a very safe procedure, though mild bleeding, infection, or nearby tissue injury can rarely occur.
Why Do People Believe Biopsy Can Spread Cancer?
This fear is understandable. Many patients hear stories such as:
| Common belief | What evidence suggests |
| “The tumor grew after the biopsy.” | The cancer may already have been growing before the biopsy. |
| “Pain or swelling after biopsy means cancer has spread.” | Mild soreness, bruising, or swelling can happen after a needle procedure and usually does not mean spread. |
| “Once cancer is touched, it becomes aggressive.” | Cancer spread depends on tumor biology, stage, and lymph or blood vessel involvement, not simply being touched. |
| “Avoiding biopsy is safer.” | Avoiding biopsy may delay diagnosis and treatment. |
Cancer can naturally spread through lymph channels, blood vessels, or nearby tissue. A biopsy is usually performed because there is already a suspicious lump or lesion that needs confirmation.
What Actually Happens During a Biopsy?
A biopsy means taking a small sample of cells or tissue from a suspicious area and sending it to a pathology lab.
For thyroid nodules, the common test is fine needle aspiration biopsy, also called thyroid FNA. A thin needle is inserted into the thyroid nodule, often with ultrasound guidance, and a small number of cells are collected for examination. Johns Hopkins Medicine notes that the sample is sent to a laboratory to check for signs of cancer.
For head and neck lumps, biopsy may include:
| Biopsy type | Common use | Key point |
| Fine needle aspiration | Thyroid nodules, neck lymph nodes, salivary gland lumps | Thin needle, usually outpatient |
| Core needle biopsy | Some larger or deeper masses | Removes a small tissue core |
| Incisional biopsy | Mouth, throat, or skin lesions | Removes part of the abnormal area |
| Excisional biopsy | Small lumps that can be removed fully | Removes the whole suspicious area |
| Endoscopic biopsy | Nose, throat, larynx, or deeper areas | Done using a scope |
The type of biopsy depends on the location, size, ultrasound appearance, and suspected diagnosis.
Why Is Biopsy So Important in Cancer Diagnosis?
Imaging tests such as ultrasound, CT scan, or MRI can show whether a lump looks suspicious. But imaging often cannot confirm cancer with certainty.
A biopsy allows a pathologist to look at cells under a microscope. This helps answer important questions:
Is it cancer or not?
What type of cancer is it?
How aggressive does it look?
Does the patient need surgery, monitoring, medicine, radiation, or another treatment?
Is more testing needed?
The American Cancer Society explains that imaging can show suspicious areas, but in many cases, biopsy is needed to make a definite cancer diagnosis.
For patients considering thyroid cancer treatment in Nepal, this step is especially important because treatment decisions depend on accurate diagnosis. A benign thyroid nodule may only need monitoring, while a malignant or suspicious nodule may need surgery or further evaluation.
Thyroid Cancer Specialist Insight: Why Thyroid Biopsy Is Usually Recommended
A thyroid cancer specialist or experienced thyroid doctor does not recommend biopsy for every thyroid nodule. Many nodules are harmless.
Usually, the decision is based on:
Thyroid ultrasound features
Size of the nodule
Growth over time
Family history
Previous radiation exposure
Suspicious lymph nodes
Voice change, swallowing difficulty, or pressure symptoms
Thyroid hormone blood tests
This is why seeing a trained thyroid doctor matters. The goal is not to biopsy everything. The goal is to biopsy the right nodules, at the right time, using the safest suitable method.
What Do Thyroid Biopsy Results Mean?
Thyroid biopsy results are often reported using the Bethesda System. This helps doctors estimate cancer risk and decide the next step.
| Bethesda result | What it means | Approximate cancer risk / next step |
| Benign | Cells look non-cancerous | Up to 70% of thyroid biopsies; malignancy risk usually less than 3%; follow-up ultrasound may be advised |
| Malignant | Cancer cells seen | About 97–99% chance it is truly cancer; surgery is usually considered |
| Suspicious for malignancy | Worrisome but not fully diagnostic | About 60–75% cancer risk; surgery often advised |
| AUS / FLUS | Indeterminate changes | About 5–15% risk; repeat biopsy or genetic testing may help |
| Follicular neoplasm | Cannot fully classify on FNA alone | About 15–30% risk; surgery may be needed for diagnosis and treatment |
| Non-diagnostic | Not enough cells | Repeat biopsy, monitoring, or surgery may be discussed |
These figures are based on patient information from the American Thyroid Association.
How Rare Is Biopsy-Related Cancer Spread?
Biopsy-related spread is possible in theory, but it is rare in real clinical practice.
The American Cancer Society says cancer spread during biopsy is extremely rare and that the benefit of biopsy usually outweighs the minimal risk.
In thyroid fine needle aspiration, needle tract implantation has been reported, but medical literature describes it as extremely rare and exceptional. Endotext, a medical reference hosted by NCBI, states that needle track implantation of thyroid carcinoma is extremely rare.
For head and neck masses, a systematic review found that seeding after fine needle aspiration or core biopsy is extremely low and should not be the deciding factor when choosing how to investigate a mass.
The key message is balanced: the risk is not zero, but it is very low. For most patients, getting a correct diagnosis is safer than avoiding biopsy because of fear.
Can Thyroid Cancer Biopsy Make Thyroid Cancer Worse?
A thyroid cancer biopsy does not make thyroid cancer biologically more aggressive.
Cancer behavior depends on factors such as:
Cancer type
Tumor size
Lymph node involvement
Tumor genetics
Age and overall health
Whether the cancer has spread before diagnosis
Papillary thyroid cancer, the most common type found in thyroid biopsies, often grows slowly. Other types, such as medullary, poorly differentiated, or anaplastic thyroid cancer, may behave differently and need faster specialist care.
A biopsy helps identify which situation the patient is facing. Without biopsy or proper evaluation, the treatment plan may be delayed or incomplete.
Why Delaying Diagnosis Can Be More Harmful Than Biopsy
Fear of biopsy can cause some patients to wait months or years before seeing a doctor. This delay can be harmful, especially when the lump is cancerous.
In Nepal, delays in cancer care are a recognized concern. The International Agency for Research on Cancer reported that many patients in Nepal may experience months of delay between first symptoms and treatment in several common cancers.
For thyroid cancer, early evaluation matters because treatment planning may include ultrasound, biopsy, surgery, lymph node assessment, radioactive iodine in selected cases, hormone therapy, and long-term monitoring.
A small neck lump should not cause panic. But it should not be ignored either.
Thyroid Cancer in Nepal: Why Awareness Matters
According to GLOBOCAN 2022 estimates, Nepal had about 22,008 new cancer cases across all cancer types in 2022. Thyroid cancer accounted for about 710 new cases, ranking eighth among listed cancer sites in the Nepal factsheet.
Globally, thyroid cancer ranked seventh in incidence in 2022, with an estimated 821,214 new cases and 47,507 deaths worldwide.
These numbers show why accurate diagnosis is important. Thyroid cancer is not the most common cancer in Nepal, but it is significant enough that patients with suspicious thyroid nodules should seek timely evaluation.
What Makes a Thyroid Biopsy Safer?
A safe thyroid biopsy depends on planning, technique, and follow-up.
Important safety steps include:
Using ultrasound guidance when needed
Choosing the correct nodule to sample
Avoiding unnecessary biopsy of clearly low-risk nodules
Reviewing blood thinner use before the procedure
Cleaning the skin properly
Using a fine needle rather than a larger instrument when appropriate
Sending samples to an experienced pathology lab
Explaining what symptoms are normal after biopsy and what needs attention
Johns Hopkins Medicine notes that ultrasound helps guide the needle to the right spot and helps prevent damage to nearby structures.
Most patients can go home the same day after thyroid FNA. Mild soreness for a day or two can happen.
When Should You See a Thyroid Cancer Specialist?
You should consider seeing a thyroid cancer specialist or experienced thyroid doctor if you have:
A thyroid nodule with suspicious ultrasound features
A lump in the neck that is growing
Hoarseness or voice change that does not improve
Difficulty swallowing or breathing
A thyroid nodule with enlarged neck lymph nodes
A family history of thyroid cancer
A previous history of radiation exposure to the neck
An indeterminate, suspicious, or malignant biopsy result
A repeat non-diagnostic thyroid biopsy
Concern about surgery or treatment planning
Dr. Prabhat Chandra Thakur is an ENT Head & Neck Surgeon/Oncosurgeon in Nepal, with training in otolaryngology-head and neck surgery, head and neck oncology fellowship, and minimally invasive thyroid surgery fellowship. (
For patients searching for thyroid cancer treatment in Nepal, a specialist can help coordinate diagnosis, surgical planning, pathology review, and follow-up.
Biopsy Myths vs Facts
| Myth | Fact |
| Biopsy always spreads cancer. | Biopsy-related spread is extremely rare. |
| A painful biopsy means cancer has spread. | Mild pain or bruising can be normal after a needle procedure. |
| Ultrasound alone can confirm cancer. | Ultrasound can suggest risk, but biopsy often confirms diagnosis. |
| All thyroid nodules need biopsy. | Many thyroid nodules only need monitoring. |
| A benign biopsy means no follow-up is needed ever. | Some nodules still need ultrasound follow-up. |
| Surgery should be done without diagnosis. | Treatment should be based on proper evaluation whenever possible. |
What Questions Should Patients Ask Before a Thyroid Biopsy?
Before a thyroid biopsy, ask your doctor:
Why do I need this biopsy?
What did the ultrasound show?
Is this nodule high-risk or low-risk?
Will ultrasound guidance be used?
What are the possible results?
What happens if the result is benign?
What happens if it is suspicious or malignant?
Do I need to stop taking any medicines before biopsy?
When will I get the report?
Who will explain the report to me?
Clear communication reduces fear and helps patients make informed decisions.
What Happens After a Thyroid Cancer Biopsy?
After biopsy, the next step depends on the report.
If the result is benign, the doctor may suggest follow-up ultrasound. If the result is non-diagnostic, repeat biopsy may be needed. If the result is indeterminate, genetic testing, repeat biopsy, or surgery may be discussed. If the result is suspicious or malignant, the doctor may recommend thyroid surgery, lymph node evaluation, or other treatment.
The American Thyroid Association notes that benign thyroid biopsy results are commonly monitored, while malignant and suspicious results often lead to surgery.
This is why biopsy is not just a test. It is a decision-making tool.
Does Every Cancer Need a Biopsy?
Not always.
Some cancers or tumors may be treated based on imaging, blood tests, endoscopy, surgical findings, or other clinical evidence. In certain situations, biopsy may be avoided if it is unsafe or unlikely to change treatment.
But for many thyroid, head and neck, breast, lung, stomach, colon, and oral lesions, biopsy is central to diagnosis.
The best decision depends on the individual case, tumor location, risk, and treatment plan.
Final Takeaway: The Truth About Biopsy and Cancer Spread
A biopsy is one of the most important tools in cancer diagnosis. It does not usually cause cancer to spread. In rare cases, tumor seeding can occur, but modern biopsy techniques and careful planning make this risk very low.
For thyroid nodules, a thyroid cancer biopsy can help separate benign nodules from suspicious or cancerous ones. This prevents unnecessary surgery in some patients and supports timely treatment in others.
Patients looking for a thyroid doctor or thyroid cancer treatment in Nepal should focus on proper evaluation, evidence-based advice, and clear discussion of risks and benefits.
Fear should not be ignored. But fear should not delay diagnosis.
FAQ: Can a Biopsy Cause Cancer to Spread?
1. Can a biopsy cause cancer to spread?
Rarely. Major cancer organizations state that biopsy-related cancer spread is extremely uncommon. The benefit of accurate diagnosis usually outweighs the small risk.
2. Is thyroid cancer biopsy safe?
Yes, thyroid fine needle aspiration is generally considered very safe. Possible risks include mild bleeding, infection, soreness, or rarely injury to nearby structures.
3. Can thyroid FNA spread thyroid cancer?
It is possible but extremely rare. Medical references describe needle track implantation of thyroid carcinoma as an exceptional complication.
4. Do all thyroid nodules need biopsy?
No. Many thyroid nodules are benign and may only need ultrasound monitoring. A doctor decides based on ultrasound features, size, symptoms, and risk factors.
5. What is the best test for thyroid cancer diagnosis?
Ultrasound is usually the first imaging test. Fine needle aspiration biopsy is commonly used when a thyroid nodule looks suspicious or meets biopsy criteria.
6. What happens if my thyroid biopsy is benign?
Most benign nodules are monitored with follow-up ultrasound. The American Thyroid Association states that benign results make up many thyroid biopsies and usually carry a low malignancy risk.
7. What if my thyroid biopsy is suspicious?
A suspicious result may need surgery, repeat biopsy, genetic testing, or specialist review. The next step depends on the Bethesda category and ultrasound findings.
8. Who should I consult for thyroid cancer treatment in Nepal?
Patients with suspicious thyroid nodules, malignant biopsy results, or neck lymph node involvement should consult a thyroid cancer specialist, ENT head and neck oncosurgeon, or thyroid surgeon experienced in cancer care.
Author Bio
Dr. Prabhat Chandra Thakur is an ENT Head & Neck Surgeon/Oncosurgeon based in Nepal. His website lists experience in oral cancer surgery, thyroid surgery, head and neck cancer surgery, endoscopic skull base surgery, and head and neck reconstruction, along with training in otolaryngology-head and neck surgery, head and neck oncology, and minimally invasive thyroid surgery.
Medical note: This article is for educational purposes only and should not replace consultation with a qualified doctor. Patients should seek personalized medical advice for diagnosis and treatment decisions.